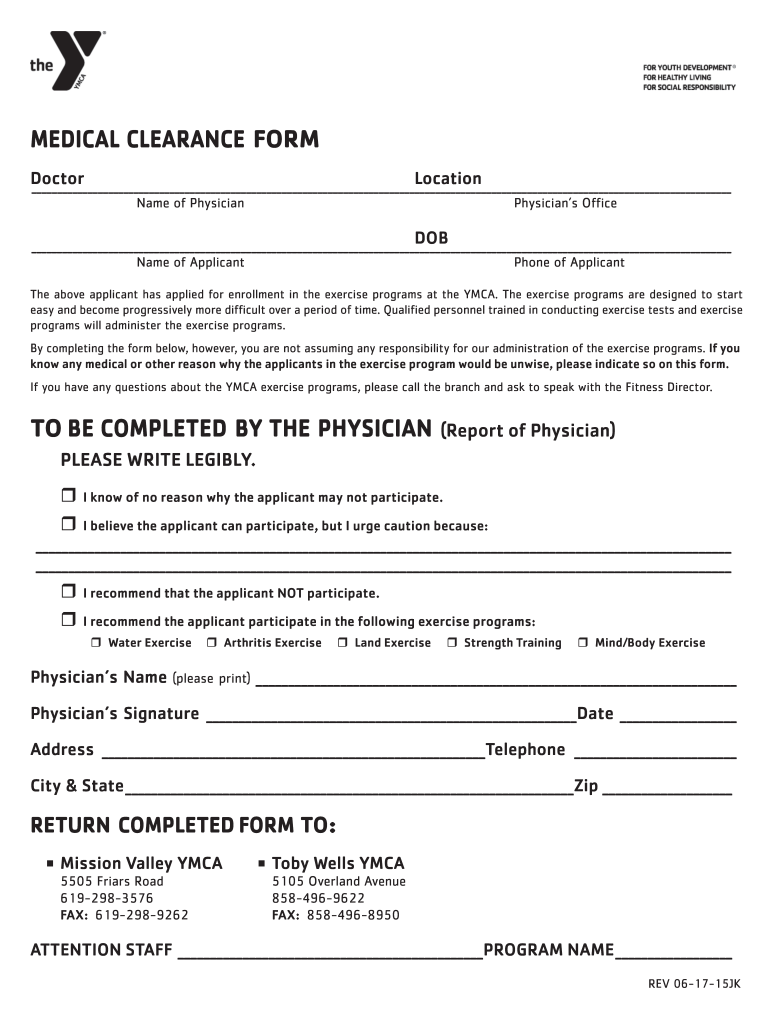
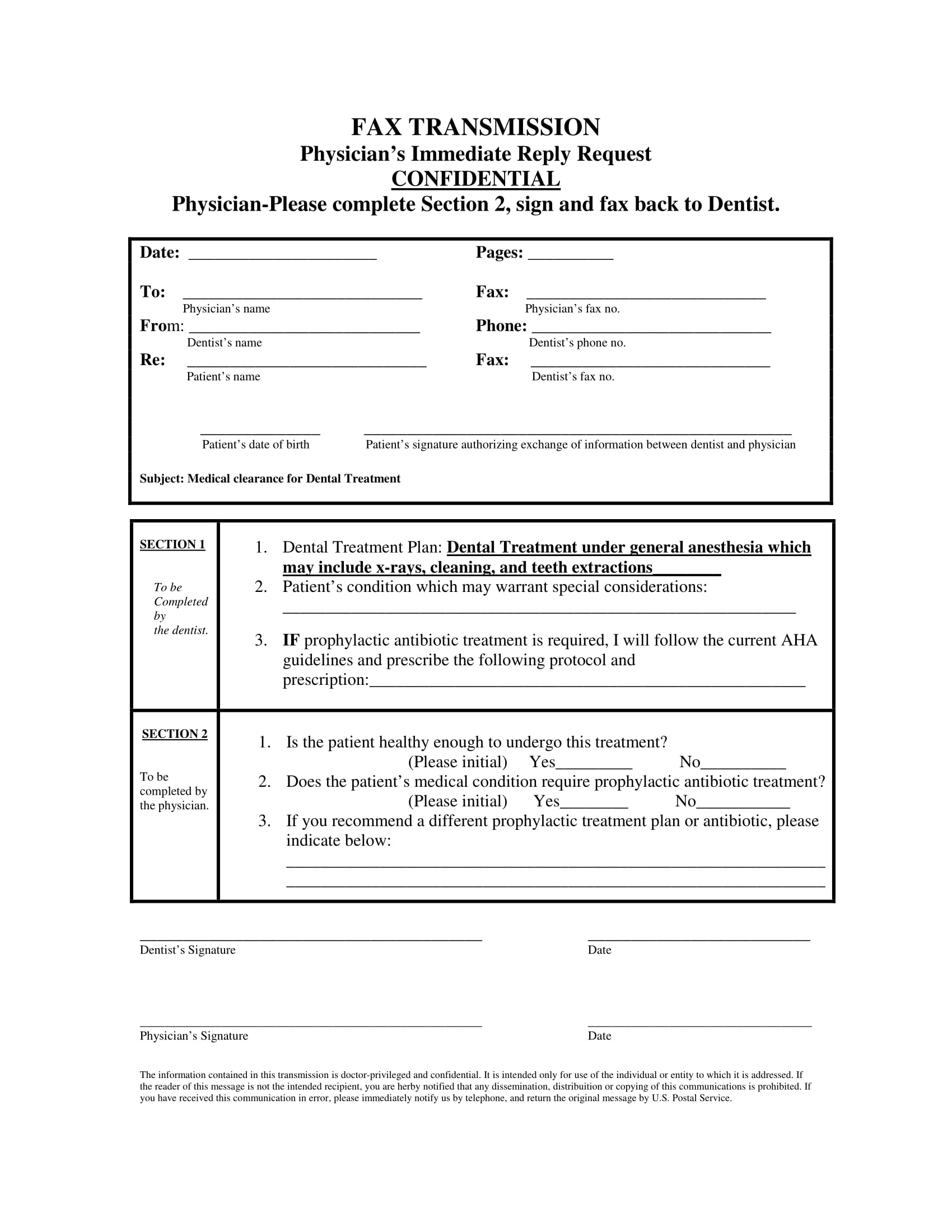
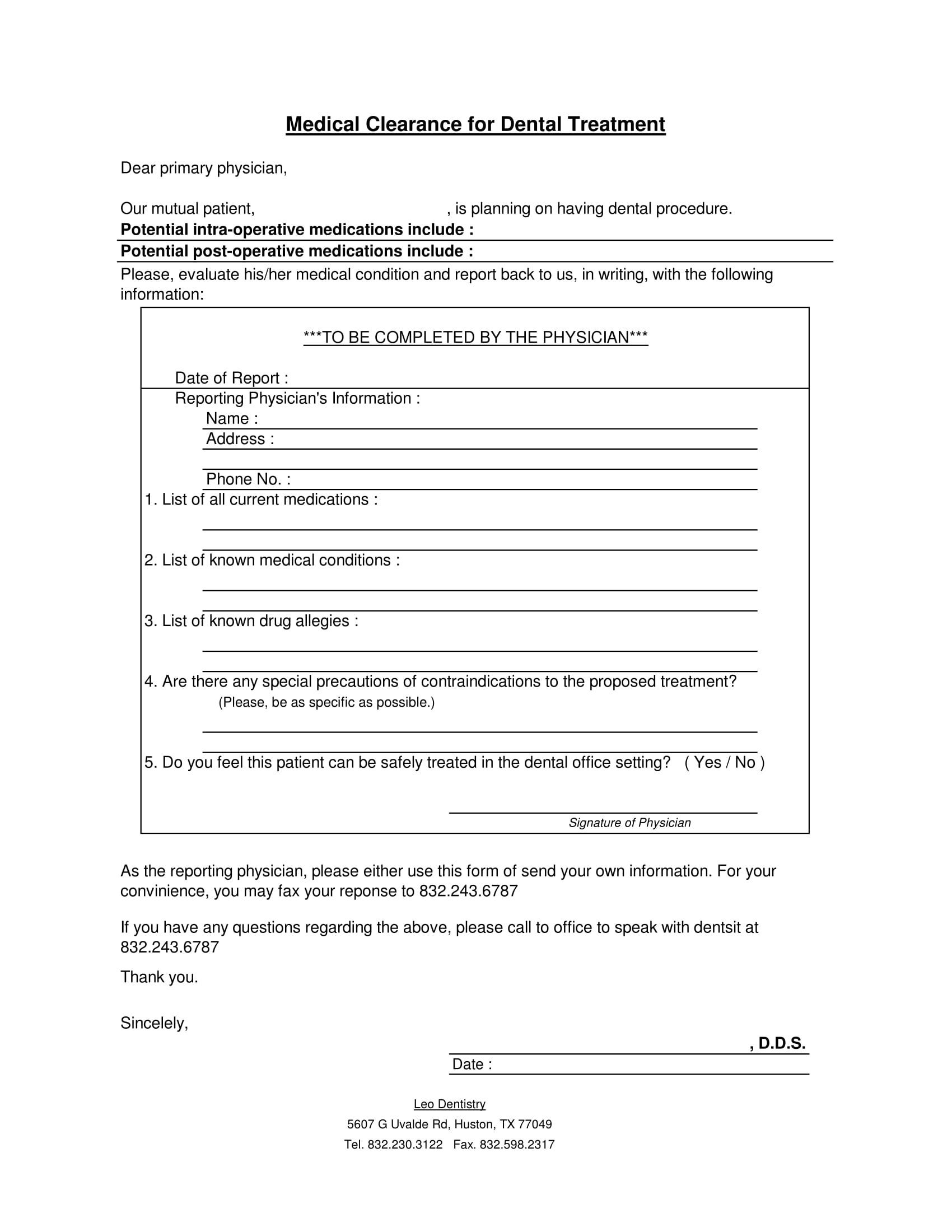
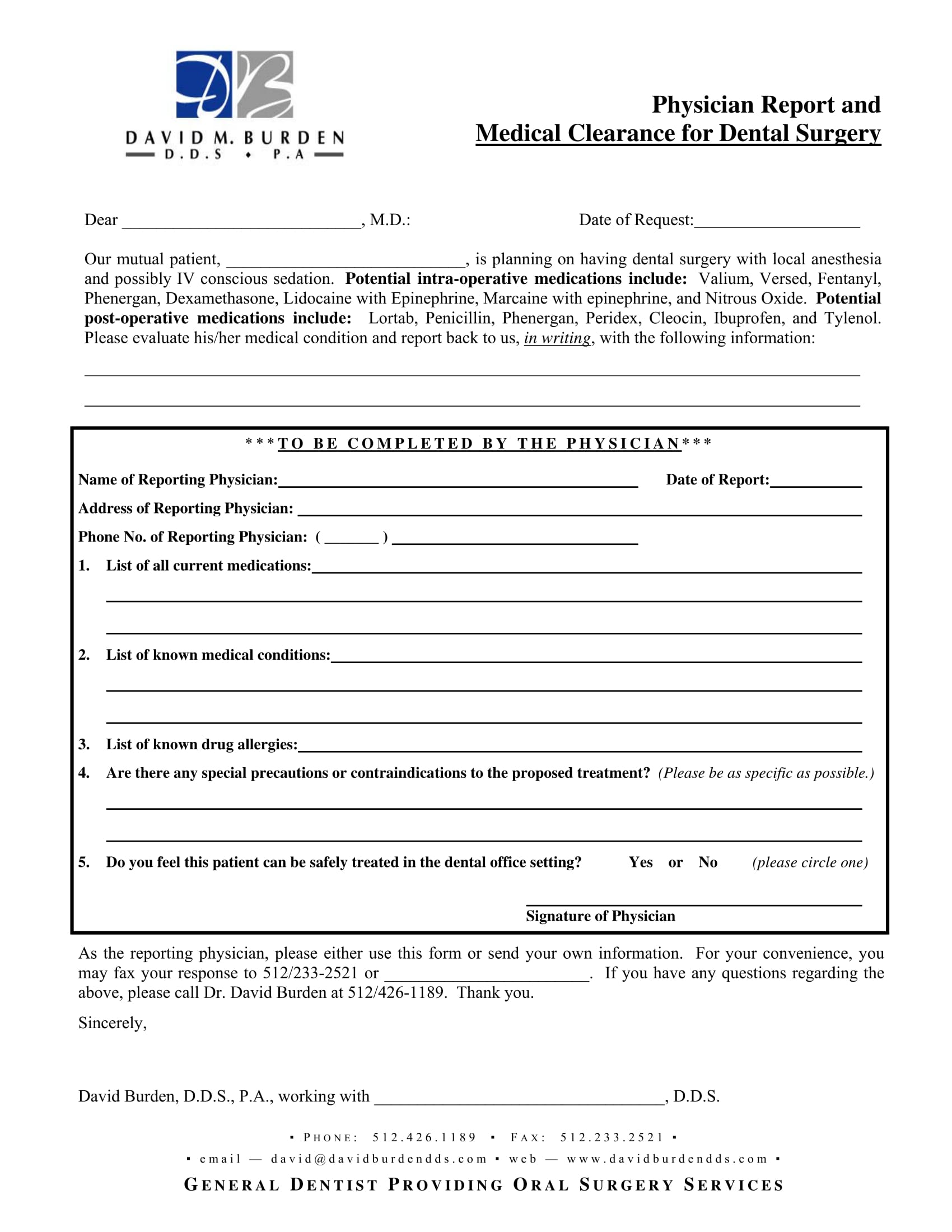
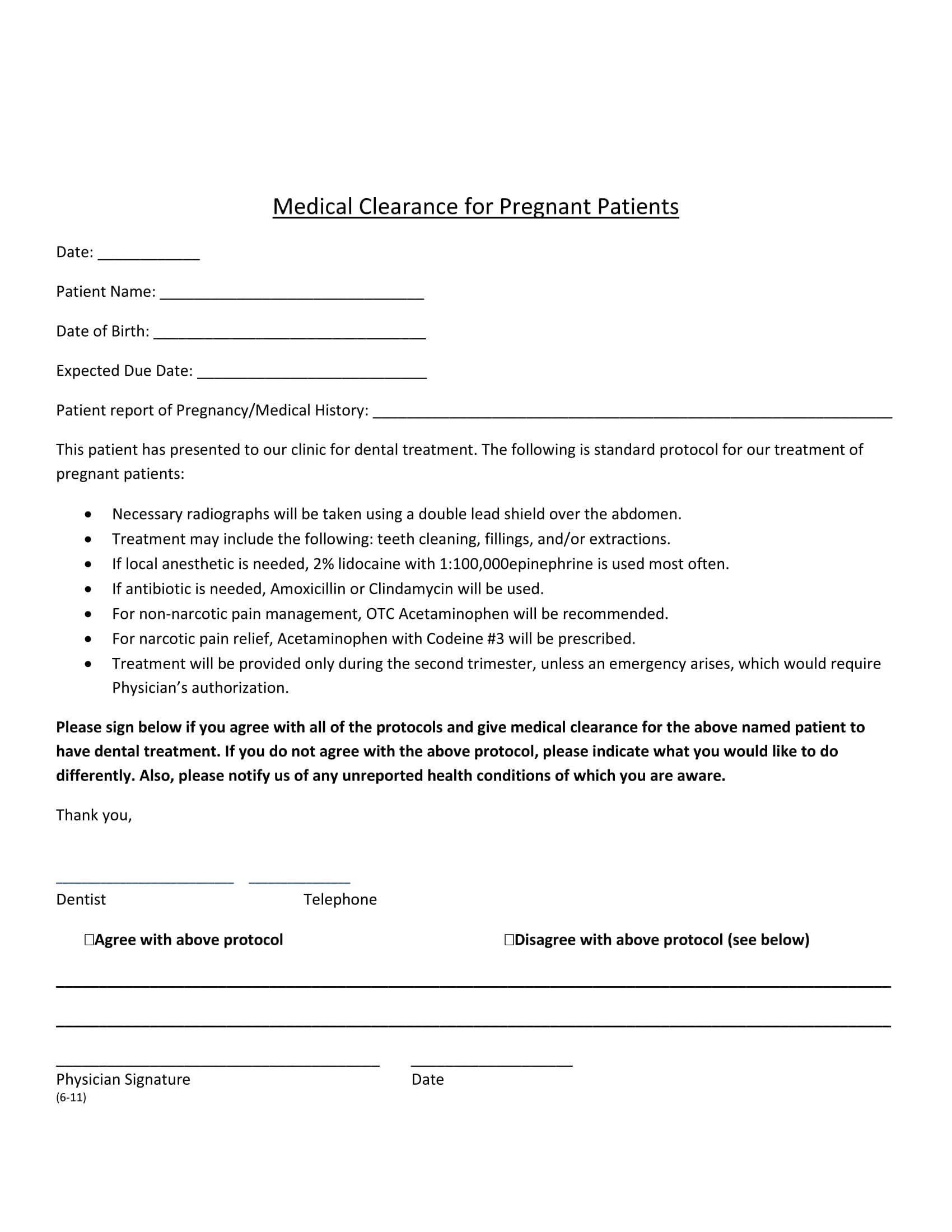
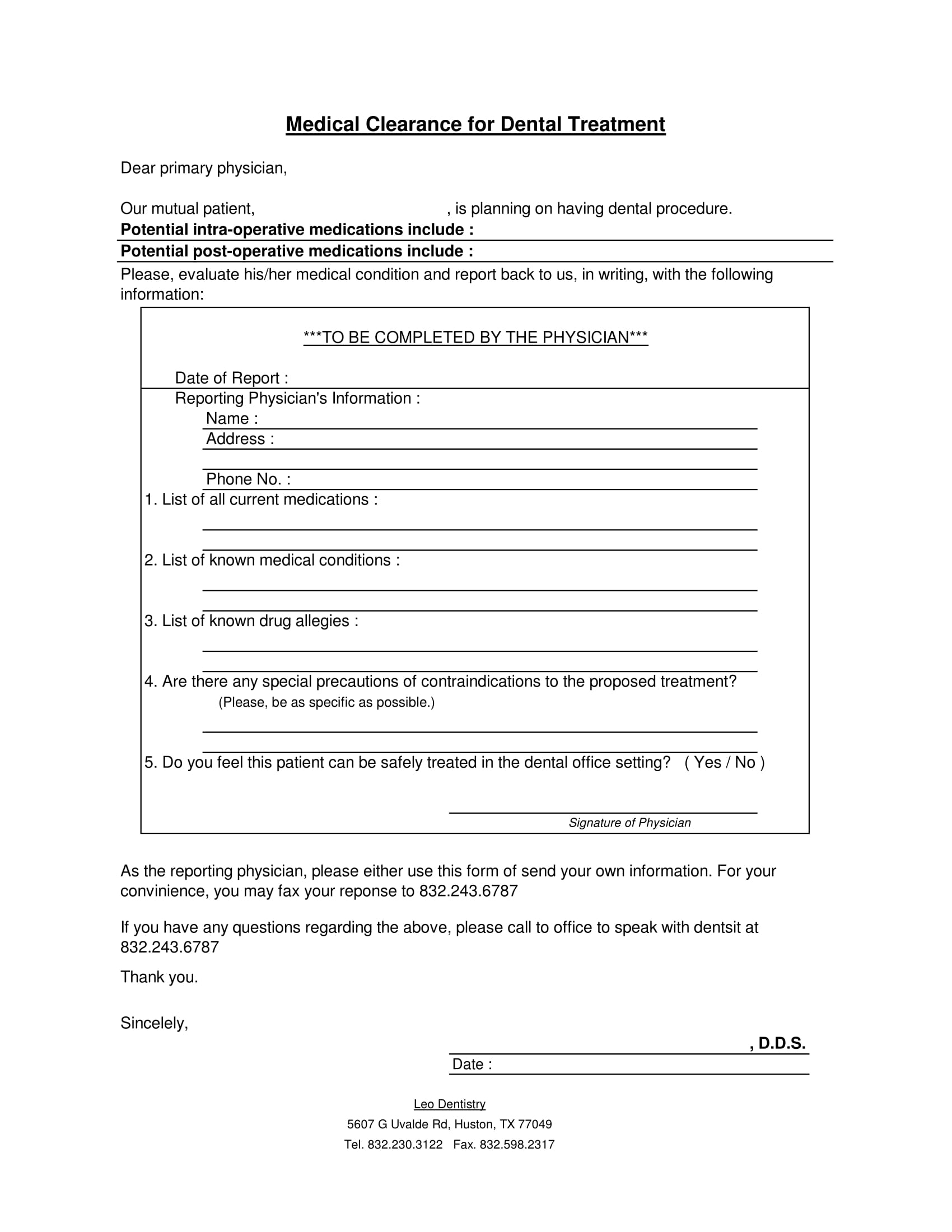
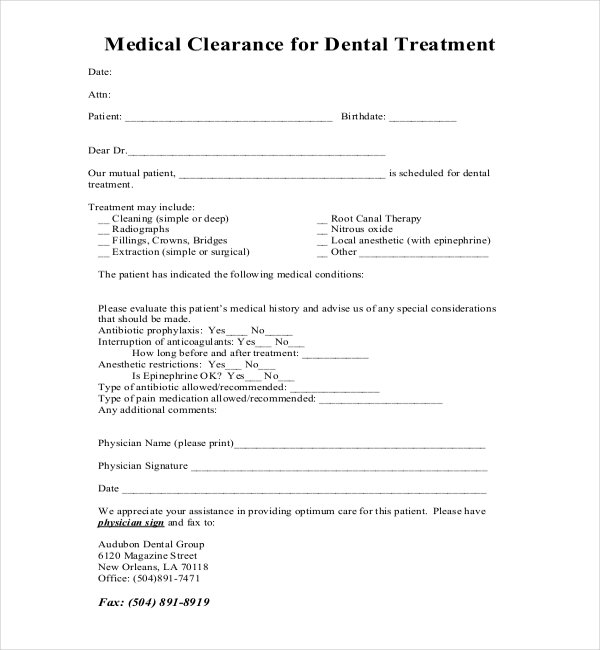
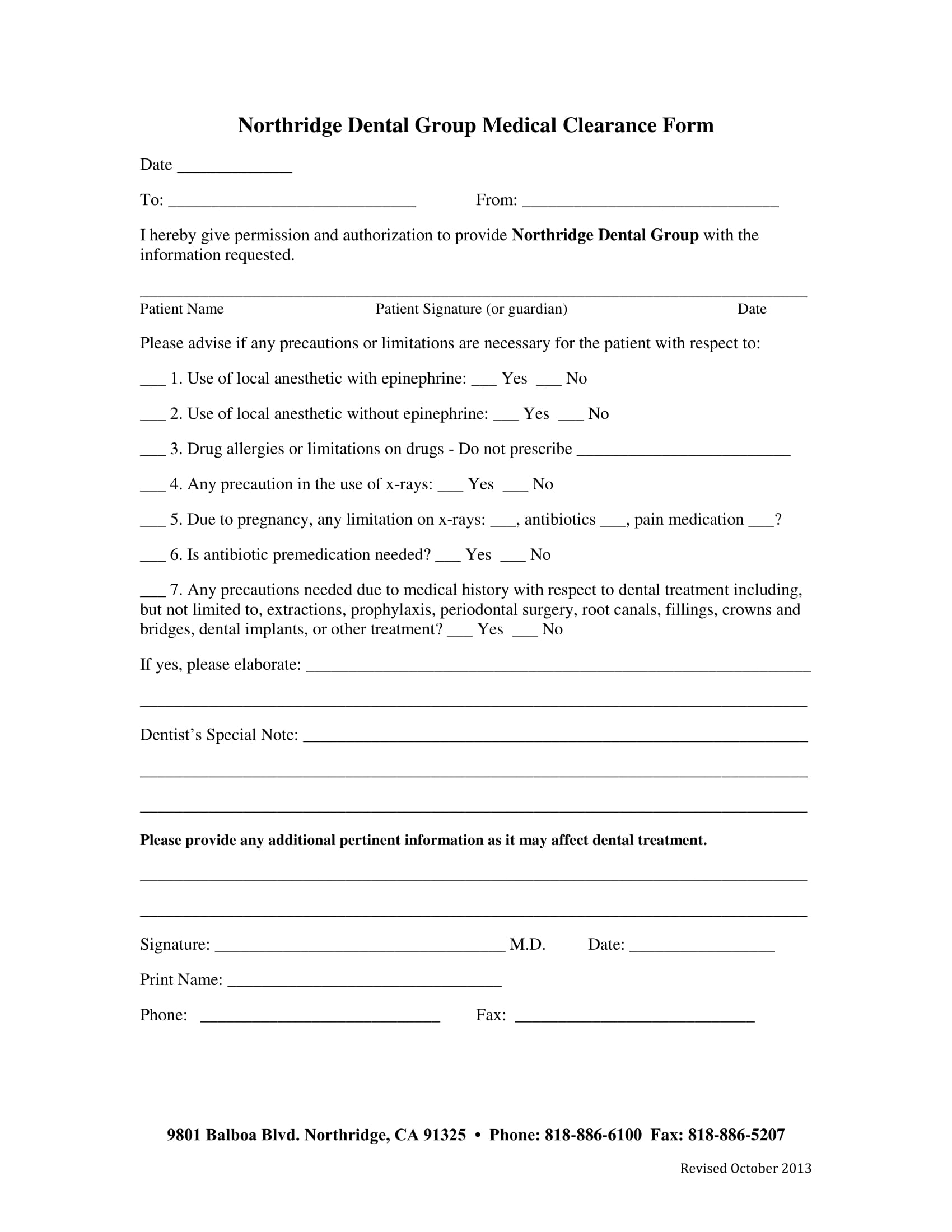
Printable Medical Clearance Form For Dental Treatment - Dental treatment that can potentially be rendered includes, but is not limited to: Medical clearance for dental treatment form. This document is essential for obtaining medical clearance prior to dental procedures. Dentist name (please print) patient signature date physicians: Please provide any information regarding the above patient's need for antibiotic prophylaxis, current cardiovascular condition, coagulation. Cleanings (prophylaxis), fluoride application, radiographs,. The patient has indicated the following medical conditions:
Dentist name (please print) patient signature date physicians: The patient has indicated the following medical conditions: Cleanings (prophylaxis), fluoride application, radiographs,. This document is essential for obtaining medical clearance prior to dental procedures. Please provide any information regarding the above patient's need for antibiotic prophylaxis, current cardiovascular condition, coagulation. Medical clearance for dental treatment form. Dental treatment that can potentially be rendered includes, but is not limited to:
The patient has indicated the following medical conditions: Cleanings (prophylaxis), fluoride application, radiographs,. This document is essential for obtaining medical clearance prior to dental procedures. Medical clearance for dental treatment form. Please provide any information regarding the above patient's need for antibiotic prophylaxis, current cardiovascular condition, coagulation. Dentist name (please print) patient signature date physicians: Dental treatment that can potentially be rendered includes, but is not limited to:

Printable Medical Clearance Form For Dental Treatment
Dentist name (please print) patient signature date physicians: The patient has indicated the following medical conditions: This document is essential for obtaining medical clearance prior to dental procedures. Medical clearance for dental treatment form. Please provide any information regarding the above patient's need for antibiotic prophylaxis, current cardiovascular condition, coagulation.
Printable medical clearance form for dental treatment Fill out & sign
Dentist name (please print) patient signature date physicians: This document is essential for obtaining medical clearance prior to dental procedures. Cleanings (prophylaxis), fluoride application, radiographs,. Dental treatment that can potentially be rendered includes, but is not limited to: The patient has indicated the following medical conditions:
Printable Medical Clearance Form For Dental Treatment Printable Word
The patient has indicated the following medical conditions: Dental treatment that can potentially be rendered includes, but is not limited to: Dentist name (please print) patient signature date physicians: Medical clearance for dental treatment form. Please provide any information regarding the above patient's need for antibiotic prophylaxis, current cardiovascular condition, coagulation.
Dental Medical Clearance Form Printable Master of Documents
Please provide any information regarding the above patient's need for antibiotic prophylaxis, current cardiovascular condition, coagulation. Dental treatment that can potentially be rendered includes, but is not limited to: This document is essential for obtaining medical clearance prior to dental procedures. Cleanings (prophylaxis), fluoride application, radiographs,. The patient has indicated the following medical conditions:
Printable Medical Clearance Form For Dental Treatment Printable Forms
Dentist name (please print) patient signature date physicians: Cleanings (prophylaxis), fluoride application, radiographs,. Please provide any information regarding the above patient's need for antibiotic prophylaxis, current cardiovascular condition, coagulation. This document is essential for obtaining medical clearance prior to dental procedures. Dental treatment that can potentially be rendered includes, but is not limited to:
Printable Medical Clearance Form For Dental Treatment
The patient has indicated the following medical conditions: This document is essential for obtaining medical clearance prior to dental procedures. Please provide any information regarding the above patient's need for antibiotic prophylaxis, current cardiovascular condition, coagulation. Dental treatment that can potentially be rendered includes, but is not limited to: Medical clearance for dental treatment form.
Printable Dental Clearance Form Printable Form 2024
Please provide any information regarding the above patient's need for antibiotic prophylaxis, current cardiovascular condition, coagulation. Medical clearance for dental treatment form. This document is essential for obtaining medical clearance prior to dental procedures. Dental treatment that can potentially be rendered includes, but is not limited to: Dentist name (please print) patient signature date physicians:
27+ Sample Medical Clearance Forms Sample Forms
Medical clearance for dental treatment form. Dental treatment that can potentially be rendered includes, but is not limited to: Cleanings (prophylaxis), fluoride application, radiographs,. This document is essential for obtaining medical clearance prior to dental procedures. Please provide any information regarding the above patient's need for antibiotic prophylaxis, current cardiovascular condition, coagulation.
Printable Medical Clearance Form For Dental Treatment Printable Forms
Please provide any information regarding the above patient's need for antibiotic prophylaxis, current cardiovascular condition, coagulation. The patient has indicated the following medical conditions: Dental treatment that can potentially be rendered includes, but is not limited to: Dentist name (please print) patient signature date physicians: Medical clearance for dental treatment form.
Printable Medical Clearance Form For Dental Treatment
Please provide any information regarding the above patient's need for antibiotic prophylaxis, current cardiovascular condition, coagulation. Medical clearance for dental treatment form. Dentist name (please print) patient signature date physicians: The patient has indicated the following medical conditions: This document is essential for obtaining medical clearance prior to dental procedures.
Cleanings (Prophylaxis), Fluoride Application, Radiographs,.
Medical clearance for dental treatment form. This document is essential for obtaining medical clearance prior to dental procedures. The patient has indicated the following medical conditions: Dentist name (please print) patient signature date physicians:
Dental Treatment That Can Potentially Be Rendered Includes, But Is Not Limited To:
Please provide any information regarding the above patient's need for antibiotic prophylaxis, current cardiovascular condition, coagulation.